
BIRTH:
In early March, I became a mama for the second time. We have nicknamed our new little one Mau Man. Our home birth didn’t feel all magical like the pictures I see on the Internet but maybe after continued exposure to oxytocin while nursing I’ll change my story and in a few years I’ll tell you all about how magical it was (feel free to call me out on it!). It was intense and brief (he came within 3 hours but it felt like days). Similar to our natural hospital birth with our first Zo, the details are hazy and I feel traumatized. Did a human just burst forth from my body? Yup! He did. Did I feel like I would give up. Heck yeah, I felt like throwing in the towel a few times, but I didn’t. Was I scared. You bet I was! Did I feel powerful afterward? You know what, I sure did! And super tired too, just like with Zo. I feel like no matter where you deliver, birth takes over you, it takes hold of your being and you just have to submit to the intensity of the process.
LOW BIRTH WEIGHT, THE CONTEXT: Now we find ourselves with our newest little one who is healthy in every single way except he was tiny at birth. 2360 grams (or 5 pounds 3 ounces). Under the low birth weight cut off of 2500 grams. I have read countless studies of how Black women like myself, regardless of socioeconomic status, are at a higher risk of pregnancy complications, maternal and fetal mortality, preterm labor and low birth weight. At my Baby Sprinkle a few months ago, a group of my closest friends and I spent considerable time discussing this topic. Pretty morbid but we are all Black doctors, educators, and health care professionals. But somehow I thought, I would be insulated, I would be spared. I took my vitamins, exercised, meditated, saw a chiropractor twice a week. With all of the complications and losses friends and patients have had I realize that low birth weight is manageable but it still hurts. After our own loss last year, I realize that regardless of how small he was I get to hold him and touch him and smell him and snuggle him and nurse him and I will do everything in my power to get his weight up.
LOW BIRTH WEIGHT, THE COMPLICATIONS: Flash forward to Day of Life 3. His weight loss was more than what our Pediatrician and I liked and he was at risk of hypoglycemia and dehydration. He had a good latch but he just couldn’t muster up enough energy to transfer milk out of my breasts fast enough to grow. I had to start nursing and feeding him every 1.5 hours and start pumping several times a day to provide expressed milk to supplement him with. We worked with an amazing local Lactation Consultant friend first at our home and then in her office and started using a Supplemental Nursing System or SNS. This is a little tube that you attach to a syringe to feed babies at the breast or using a finger to help train them. This helps prevent nipple confusion by delaying the introduction of a bottle. Day of Life 4 was a blur with a ton of feeding and pumping. Day of Life 5 - he had begun to gain weight and his parents were exhausted. We were allowed to space him out to every 2 hour feeds. Day of Life 9 back to birth weight. Day of life 18 weight up to 6 pounds.
And this is where we find ourselves: Nurse and reposition the SNS 10 times. Pump. O finger feeds with SNS in the early evening so that I can sleep for a few hours (this is priceless! Many thanks to Lactation and our old school Pediatrician who made this a key part of our process). Smile. Cry. Have a melt down feeling guilty that I couldn’t make him fatter. Listen to a podcast. Take a lactation supplement. Play with Zo for a few minutes. Tell Zo to be gentle and not climb on me while I’m nursing. Get a pep talk from the hubby. Repeat.
I’ll keep you posted and can’t wait until I can throw this SNS out. I pray for the day he is exclusively breast fed and that breastfeeding soothes him.
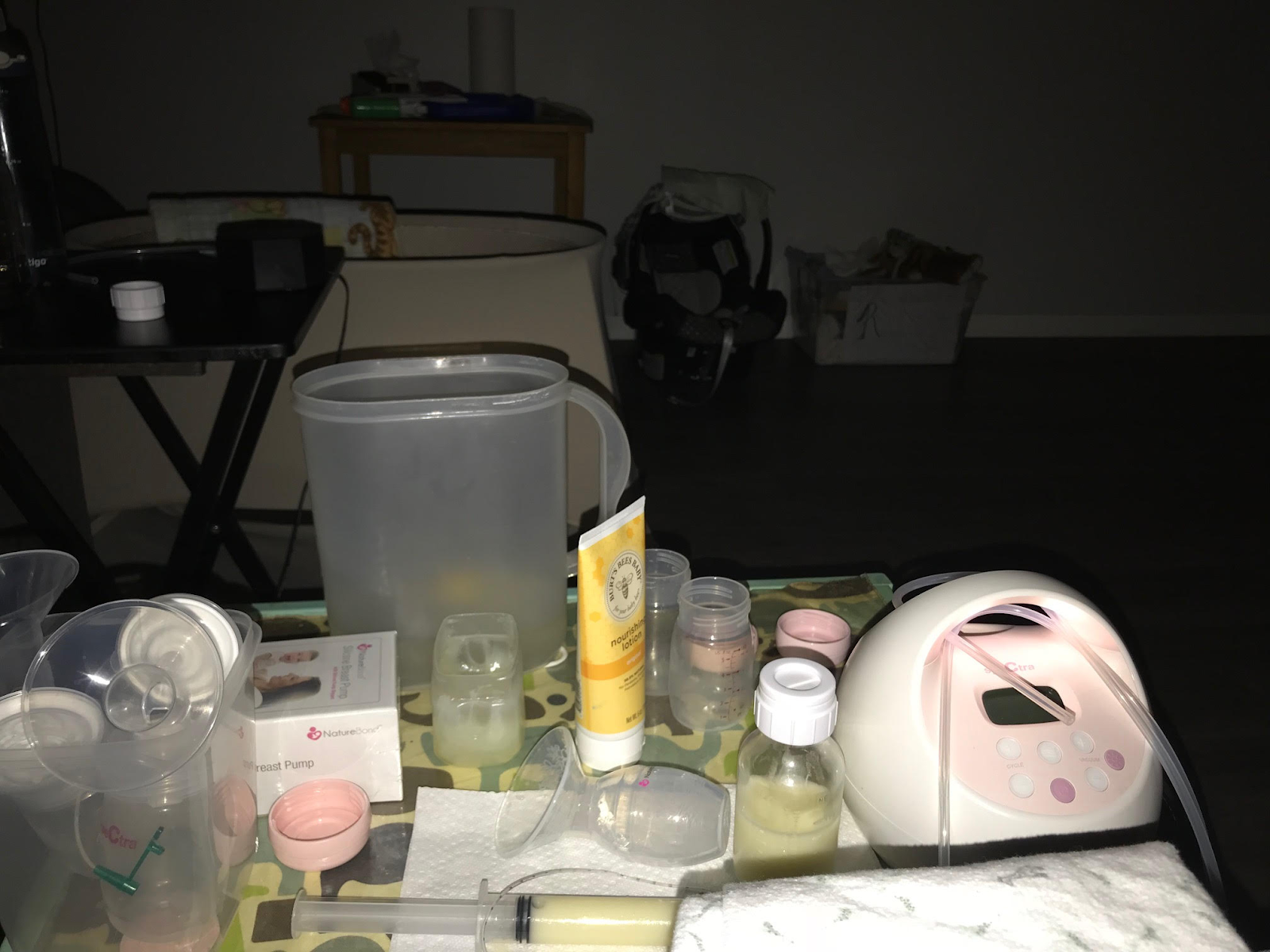 |
| My world at night: our 30mL syringe, the SNS premature baby feeding tube, my 2 pumps - my Spectra electric pump for daytime pumping and my NatureBond silicone manual suction pump for easy night time pumping - I pop it on the alternate breast while nursing/SNS feeding. |
REFERENCES:
Adverse birth outcomes in African American women: the social context of persistent reproductive disadvantage. https://www.ncbi.nlm.nih.gov/pubmed/21213184
Black Women Disproportionately Suffer Complications of Pregnancy and Childbirth. Let’s Talk About It. https://www.propublica.org/article/black-women-disproportionately-suffer-complications-of-pregnancy-and-childbirth-lets-talk-about-it
Racial Discrimination and Adverse Birth Outcomes: An Integrative Review. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5206968/
What’s Killing America’s Black Infants? Racism is fueling a national health crisis. https://www.thenation.com/article/whats-killing-americas-black-infants/
